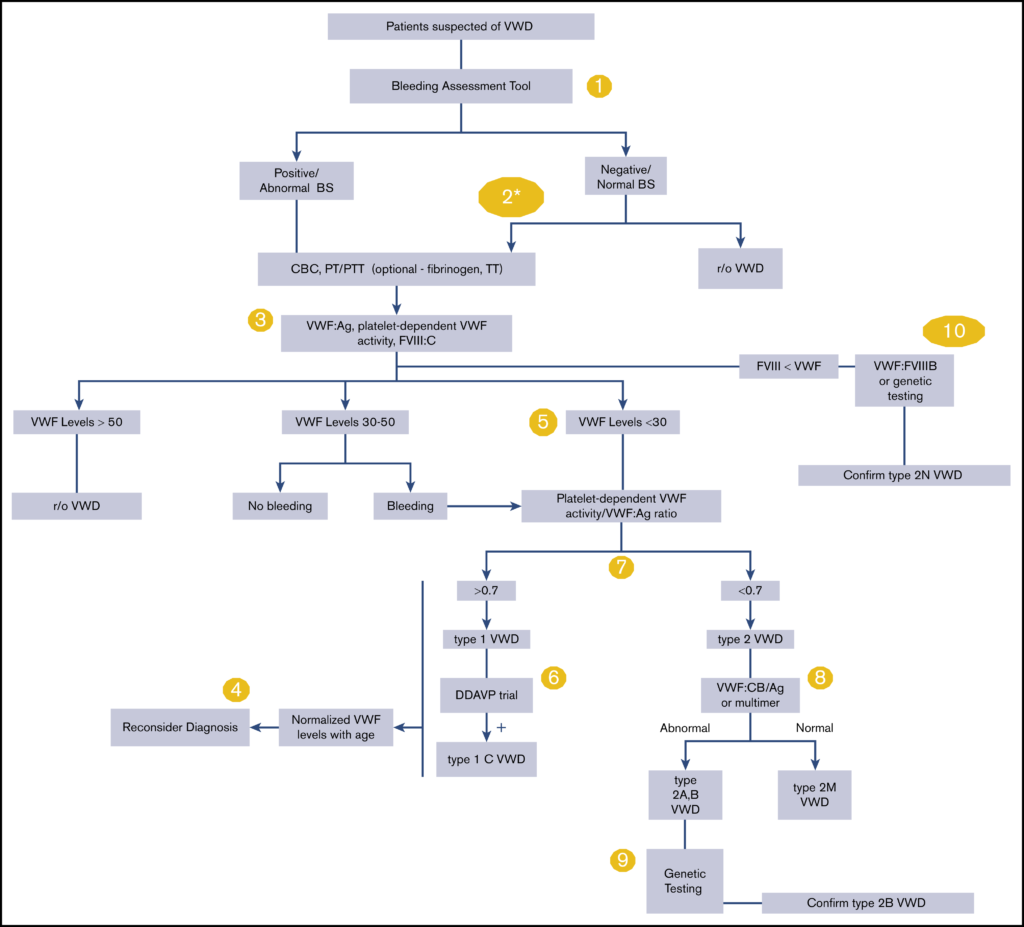
Von Willebrand disease (VWD) is the most common hereditary bleeding disorder globally. Currently, VWD is classified as either type 1, 2 or 3, characterised by quantitative and qualitative deficiencies in von Willebrand factor (VWF). As such, the severity of bleeding can differ between types. Symptoms can include excessive mucocutaneous bleeding, epistaxis, heavy menstrual bleeding for women, prolonged bleeding from minor wounds and gastrointestinal bleeding. Developed from systematic evidence reviews from the Outcomes and Implementation Research Unit at the University of Kansas Medical Center (KUMC), the American Society of Haematology (ASH), in collaboration with the National Haemophilia Foundation (NHF) and the World Federation of Haemophilia (WFH), have developed updated guidelines for the diagnosis of VWD. Figure 1 details the algorithm for diagnosis, with specific recommendations corresponding to each number in the algorithm. Recommendations that are suggested are done so based on low certainty in the evidence behind the specific recommendation.
Summary of recommendations
For patients with a low probability of VWD, a validated bleeding-assessment tool (BAT) is recommended as an initial screening tool to identify which patients required specific blood testing over non-standardised clinical assessment. Specific blood testing for VWD refers to VWF antigen (VWF:Ag), platelet-dependent VWF activity (eg, VWF glycoprotein IbM [VWF:GPIbM]), and factor VIII coagulant activity (FVIII:C).
For patients with an intermediate probability of VWD, BAT should not be relied upon when deciding if a patient requires further specific blood testing. Intermediate probability is defined as patients typically presenting with an abnormal bleeding history or abnormal initial laboratory tests.
For patients with a high probability of VWD, BAT should not be relied upon when deciding if a patient requires further specific blood testing. High probability patients are typically those with a first-degree relative with VWD, regardless of their bleeding symptoms or initial laboratory results.
Newer assays, that measure the platelet-binding activity of VWF, for e.g VWF:GPIbM, VWF:GPIbR, should be used over the VWF ristocetin cofactor assay (VWF:RCo) for the diagnosis of VWD.
The diagnosis of patients with type 1 VWD should be reconsidered, rather than removed, if the patient’s VWF levels have normalised with age. Aging and comorbidities are known to increase VWF levels, although the association of increased VWF levels and bleeding symptoms, in the setting of a VWD diagnosis is not established.
A VWF levels of <0.30 IU/mL regardless of bleeding symptoms, and a VWF of <0.50 IU/mL with abnormal bleeding, should be used to confirm a diagnosis of type 1 VWD. This refers to VWF levels obtained from VWF:Ag and/or platelet-dependent VWF activity (eg, VWF:GPIbM). Furthermore, the lower limit of the normal range defined by the local laboratory should be used, if it is <0.50 IU/mL. VWF is a dynamic reactant and diagnostic testing should be performed when the patient is at a baseline state of health.
For the diagnosis of type 1C VWD, a trial of desmopressin is suggested, with 1- and 4-hour post-infusion blood work to confirm increased VWF clearance, as opposed to VWF propeptide (VWFpp)/VWF:Ag testing.
When type 2 VWD is suspected, it is suggested that a platelet-dependent VWF activity/VWF:Ag ratio <0.7 be used as a cut-off, rather than <0.5, for patients with an abnormal initial VWD screen. This is because some type 2 VWD patients can have a normal VWF:Ag and platelet-dependent VWF activity but a low ratio of platelet-dependent VWF activity/VWF:Ag.
It is also suggested that if additional testing is required for the diagnosis of type 2A, 2B or 2M VWD, that VWF multimer analysis or VWF collagen binding (VWF:CB)/VWF:Ag (the ratio of VWF collagen binding to antigen) be used.
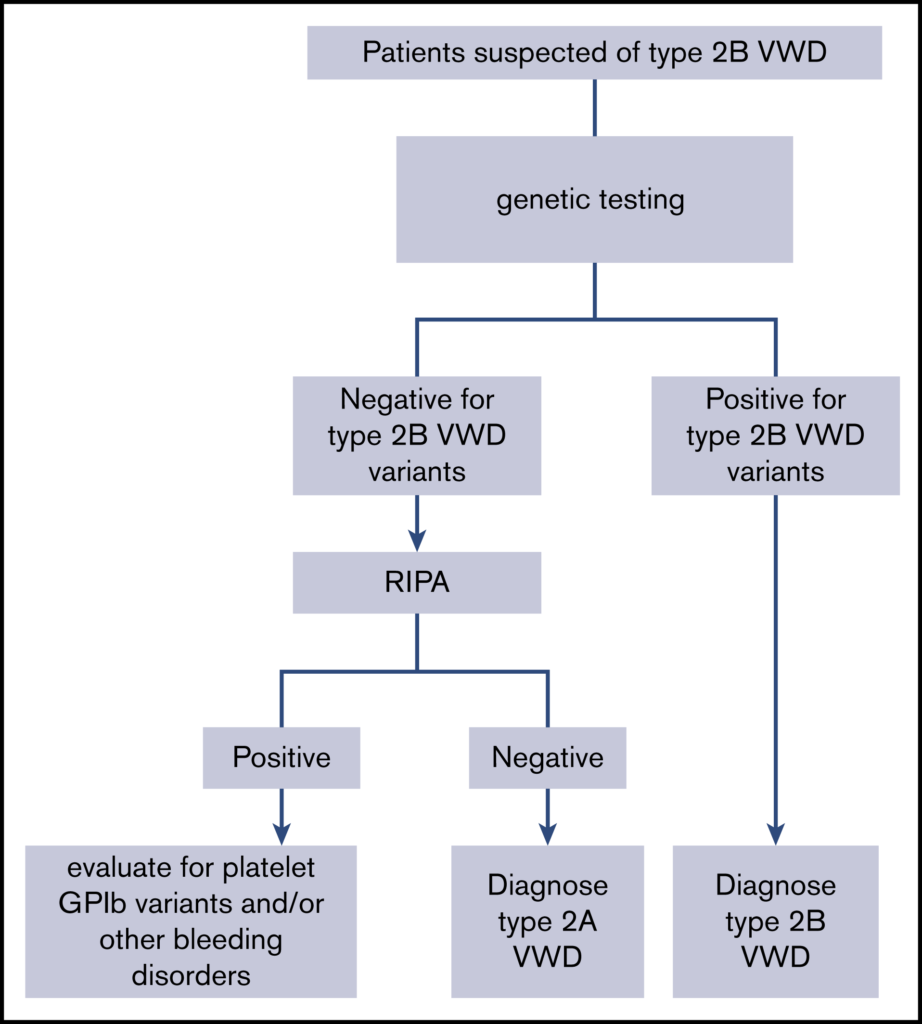
If additional testing is required for the diagnosis of type 2A or 2B VWD, targeted genetic testing is suggested over low-dose ristocetin-induced platelet agglutination (RIPA) (Figure 2).
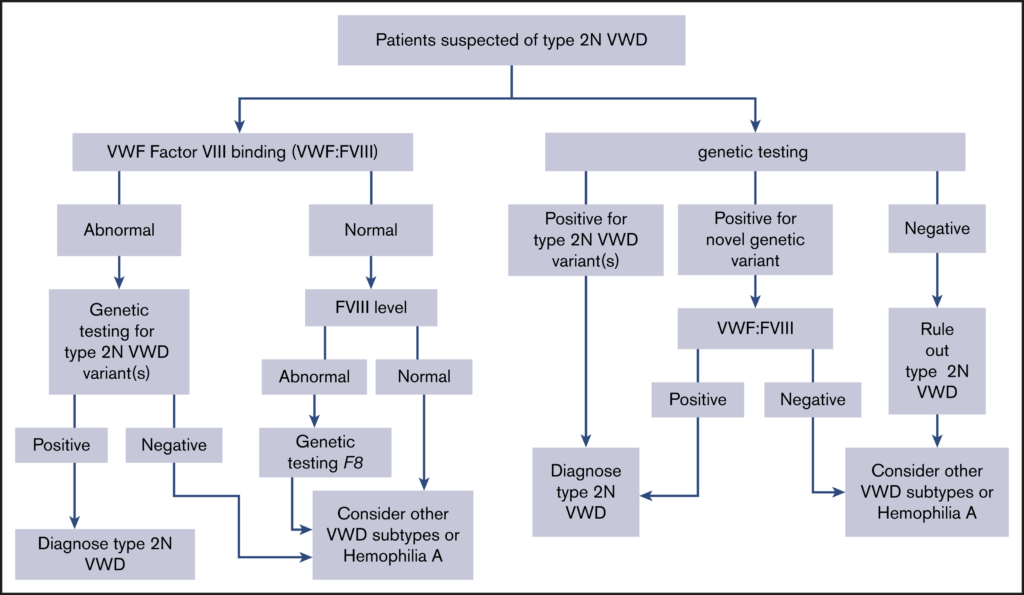
Finally, it is suggested to use either VWF FVIII binding (VWF:FVIIIB) or targeted genetic testing for the diagnosis of type 2N VWD that requires additional testing (Figure 3).
Figure 1: An overall algorithm for addressing the diagnosis of VWD.
Figure 2: An algorithm for the diagnosis of type 2B VWD.
Figure 3: An algorithm for the diagnosis of type 2N VWD.